ALERT:Be aware of fraudulent job offers using the Cerium Pharmaceuticals name.More Information.
Primary Membranous Nephropathy
What is PMN?
Membranous nephropathy (MN) is a frequent cause of nephrotic syndrome (NS) in nondiabetic adults.Eighty percent of MN is classified as PMN (also referred as idiopathic membranous nephropathy), a kidney-specific autoimmune glomerular disease, more specifically referred to as a podocytopathy; 20% of MN is classified as secondary, due to a variety of other illnesses.
An Autoimmune Disease
PMN is a disease with relatively slow progression.One-third of patients will go into spontaneous remission even without any treatment; one-third will have persistent proteinuria with long-term preservation of renal function; and one-third will have a disease progressing to renal failure (Cattran et al. 2017, Ponticelli et al. 2020).
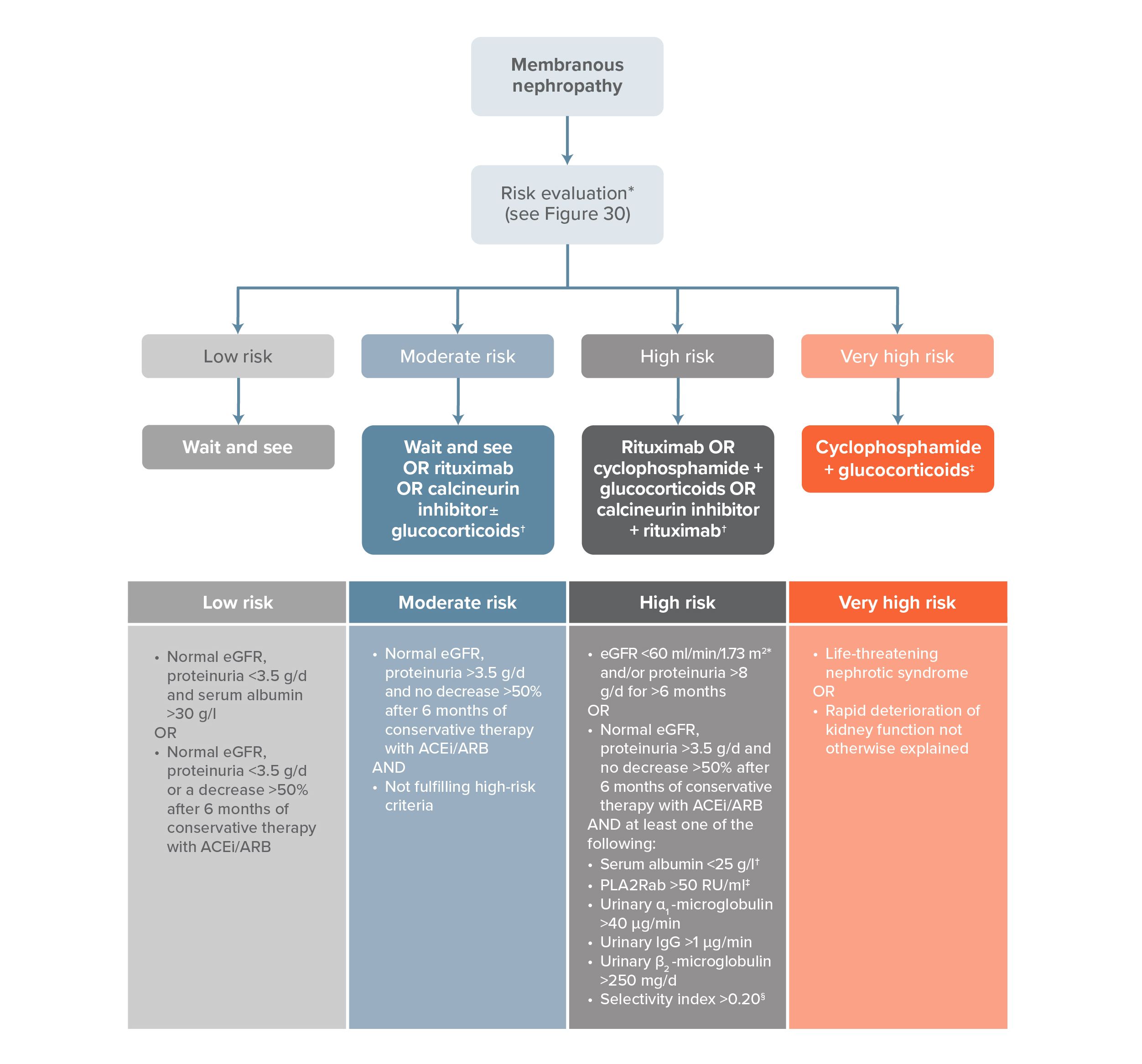
Per the Kidney Disease Improving Global Outcomes [KDIGO] Guidelines (2020), initial therapy for PMN should be supportive and involves restricting dietary protein intake and controlling blood pressure, hyperlipidemia, and edema (Figure 1).
Figure 1
Risk-based Treatment of PMN: KDIGO Clinical Practice Guideline on Membranous Nephropathy
These nonsteroidogenic actions of ACTH and ligands for the same melanocortin receptors mediate important mechanisms of actions of ACTH and ACTH-like peptides, in addition to the steroidogenic activity of ACTH described many years ago. ACTH binds to the melanocortin 2 receptor (MC2R) in the adrenal gland, and it also binds to all melanocortin receptors increasing cyclic adenosine monophosphate (cAMP) production.
Adding a treatment option, like long-acting synthetic ACTH therapy supported by the strongest published total response rate against PMN, would be a valuable addition to the arsenal of clinicians for the treatment of PMN.